Femoroacetabular impingement (FAI) is caused by reduced clearance between the femoral head and acetabulum due to anatomic abnormalities of the femur (cam FAI), acetabulum (pincer FAI), or both (mixed FAI). Cam FAI is characterized by an aspherical femoral head or reduced femoral head-neck offset. During hip flexion, the abnormally shaped femur may cause shearing at the chondrolabral junction, thereby damaging articular cartilage and the acetabular labrum. Currently, diagnosis of cam FAI is largely accomplished using two-dimensional (2D) measurements of femur morphology acquired from radiographic projections or a series of radial planes from computed tomography (CT) or magnetic resonance (MR) images. Two- dimensional measures provide initial diagnosis of cam FAI, but their reliability has been debated. Also, there is no agreement on the range of measurements that should be considered normal. Furthermore, radiographic measures give only a limited description of femur anatomy or shape variation among cam FAI deformities. Together, these limitations of 2D measurements translate into a high misdiagnosis rate. In a series of FAI patients treated with surgery in our clinic, 40% had seen multiple previous musculoskeletal providers and 15% had undergone surgical procedures unrelated to the hip joint (hernia, etc.).
|
|
| Mean control (left) and cam (right) shapes. Middle images show the mean control shape with color plots depicting how the mean cam shape differed across the femoral head, neck, and proximal shaft. Top and bottom rows show different rotations of the femoral head. |
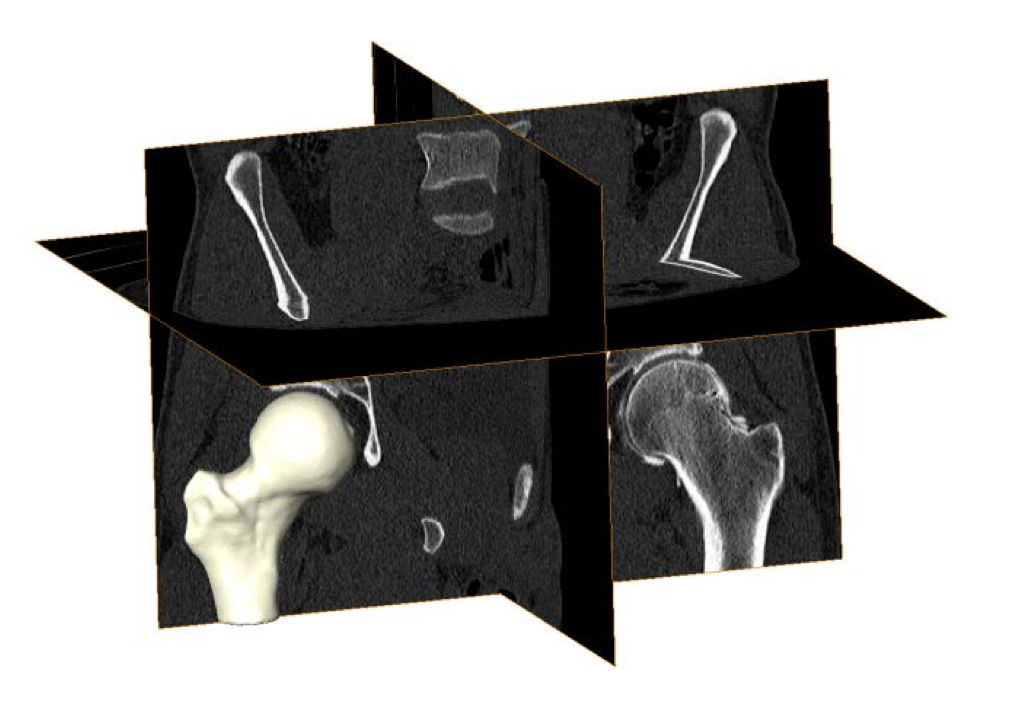
Volumetric CT images from a cam FAI patient. Validated threshold settings were applied to CT images to segment and reconstruct the bony morphology of each femur. |